
ProZema is a probiotic blend taken orally to reduce the symptoms of atopic dermatitis and eczema in children 4-17 years old. Probiotics are live microorganisms that can provide health benefits for patients who have an imbalance of bacteria. Prozema uses a blend of three patented probiotic strains, Bifidobacterium lactis CECT 8145, Bifidobacterium longum CECT 7347, and Lactobacillus casei CECT 9104. These probiotic strains have shown the highest efficacy in a meta-analysis study of randomized controlled studies for oral probiotics treating pediatric atopic dermatitis.
ProZema contains 30 doses in powder form for convenience. It is tasteless and odorless, ideal for mixing with drinks and food, and easy to schedule. ProZema should be taken for three months for best results.
ProZema complements eczema and atopic dermatitis treatments.
Atopic dermatitis and eczema manifest on the skin as redness, itchiness, or scaling, but the disease doesn’t originate at the skin’s surface. Atopic dermatitis is immunological and is related to other atopic disorders like asthma and allergic rhinitis.
Recent research has shown that intestinal barrier function problems owing to a lack of healthy microbiomes may be linked with atopic dermatitis. Lack of gut bacteria diversity may lead to pro-inflammatory conditions in the gut, leading to loss of barrier integrity. In a randomized double-blinded clinical trial, 96% of patients in the probiotic group improved their SCORAD values, measuring the severity of atopic dermatitis symptoms. After 12 weeks, the probiotic group outperformed the placebo group in SCORAD, eczema spread, eczema intensity, and subjective symptoms (such as itch and sleeplessness).
Probiotics may help reduce allergic hypersensitivities by regulating the Th2 mediated response. However, the effect of probiotics is strain-dependent, so it isn’t sufficient to take any probiotic product as a cure-all. Similarly, probiotics can exhibit different properties when combined with other strains.
Two critical studies provide explicit support for ProZema’s approach.
Study 1: Meta-analysis of probiotic strains used to treat pediatric atopic dermatitis
Meta-analysis is a statistical analysis of the high-quality studies in a field and is widely considered the most robust source of evidence. It aggregates information, adding greater statistical reliability, and is especially critical in adding confidence to a relatively new field like probiotics.
This particular study aims to synthesize the available evidence, comparing the effectiveness of different probiotic preparations. The outcomes measured include relief of atopic dermatitis symptoms using SCORAD and any developments of adverse events such as fungemia, sepsis, and gastrointestinal ischemia.
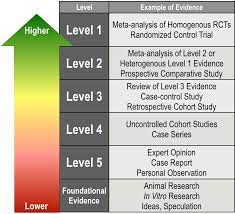
Methodology: Search for all randomized control trials from inception until Jan 31, 2020, published on Cochrane Library, MEDLINE, TRIP Database, Center for Reviews and Dissemination that meet criteria.
Results and Discussions: 6 strains of probiotics performed better than placebo. Mix 1 (Bifidobacterium animalis subsp lactis CECT 8145, Bifidobacterium longum CECT 7347, and Lactobacillus casei CECT 9104), in particular, showed the most significant reduction of atopic dermatitis symptoms with high certainty of evidence.
Study 2: Oral Probiotic Mix for Young Patients With Moderate Atopic Dermatitis
This study is a 12-week randomized, double-blind, placebo-controlled intervention trial in Spain (March to June 2016) designed to evaluate the influence of probiotics on atopic dermatitis symptoms and the use of topical steroids in children. The probiotic mix (Bifidobacterium lactis CECT 8145, Bifidobacterium longum CECT 7347, Lactobacillus casei CECT 9104) scored highest in the meta-analysis in study 1 and is the same probiotic mix used in ProZema.
Methodology: 12-week randomized, double-blind, and placebo-controlled intervention trial. Children aged 4-17 years old, excluding those having undergone systemic immunosuppressive drugs in the three months prior to the study or those diagnosed with intestinal bowel disease or bacterial infection. Patients were given a daily maltodextrin capsule for 12 weeks, separated into the probiotic arm (Bifidobacterium lactis CECT 8145, B longum CECT 7347, and Lactobacillus casei CECT 9104) and the placebo control arm (maltodextrin only).
SCORAD index score and days of topical steroid use were recorded. SCORAD is a clinical measurement of atopic dermatitis symptoms that are scored based on the percentage of the skin’s surface area affected, the severity of the symptom, and subjective symptoms such as itch and sleeplessness. The study aims to measure the efficacy of the probiotic mix in pediatric patients with moderate atopic dermatitis. The probiotic mix used contains the following strains:
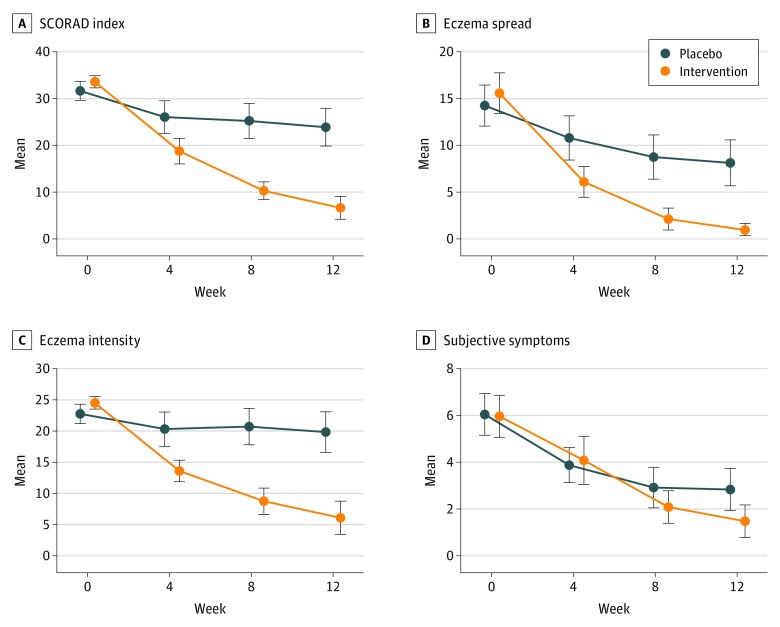
Figure 2. Change in SCORAD and Its Components, Navarro-López V et al. JAMA Dermatol. 2018; 154 (1):37-43
Results and Discussion: The probiotic mix group outperformed the placebo group in the SCORAD index by a statistically significant margin and used less steroids. Antibiotic use, diet, and other concomitant allergies were controlled for. Administering this mixture of probiotics as an adjunctive treatment may be effective in reducing SCORAD, and thereby reducing steroid use due to atopic dermatitis flares.
22 of 23 patients in the probiotic group (96%) improved in the SCORAD index. In comparison, only 11 in the placebo group improved (46%). The probiotic group also had fewer days of steroid use (336 patient-days) than the placebo arm (291 patient-days).
Other Findings:
Atopic dermatitis is the most common form of eczema, and is extremely common in children. It affects up to 25% of children and up to 10% of adults. While many children eventually “outgrow” the condition, others will live with atopic dermatitis in adulthood. There is no cure at this time. The exact mechanisms of atopic dermatitis aren’t yet understood, but there is growing evidence that it is autoimmune in origin.

Atopic dermatitis often affects the flexural areas. Source: Eczemaguide.ca
Atopic dermatitis is characterized by redness, itch, and dryness of the skin. The symptoms can be local or widespread, and there is a wide range of severity. Atopic dermatitis waxes and wanes. During a flare, the symptoms quickly worsen, followed by a recovery or remission period where the symptoms are milder.
Called the itch-scratch cycle, atopic dermatitis can cause severe itching, which prompts scratching, which damages the skin, making atopic dermatitis worse. It can be difficult to stop scratching, and it can even occur during sleep. The itch-scratch cycle can cause atopic dermatitis symptoms to worsen very quickly during a flare-up, and can keep children awake at night, hindering their quality of life significantly.
While atopic dermatitis has a strong genetic component, environmental factors play a major role in triggering flare-ups. Proper skincare routines, moisturizing, and avoiding potential triggers like harsh soaps and detergents can help minimize flare-ups. During flare-ups, controlling the symptoms quickly is the best way to keep the itch-scratch cycle from worsening the underlying disease.
The first line of treatment for atopic dermatitis is topical steroids. It is fast-acting and reduces inflammation effectively. Calming inflammation quickly is critical as patients will scratch the skin if itching remains uncontrolled, which will worsen the symptoms through the itch-scratch cycle.
The one drawback with steroids is that, when strong steroids are used for too long, they can have negative side-effects, so doctors are careful to prescribe the right strength, and often use it in conjunction with other therapies.